endovasculares.es




Noticias

- Título: Women cardiologists do different work, make less money than men
- Fecha: 09-11-2015
DURHAM, N.C. -- Despite efforts to increase gender diversity in cardiology, major differences in job characteristics and pay persist between men and women who treat heart patients, according to a Duke Medicine-led study presented at the annual American Heart Association meeting.
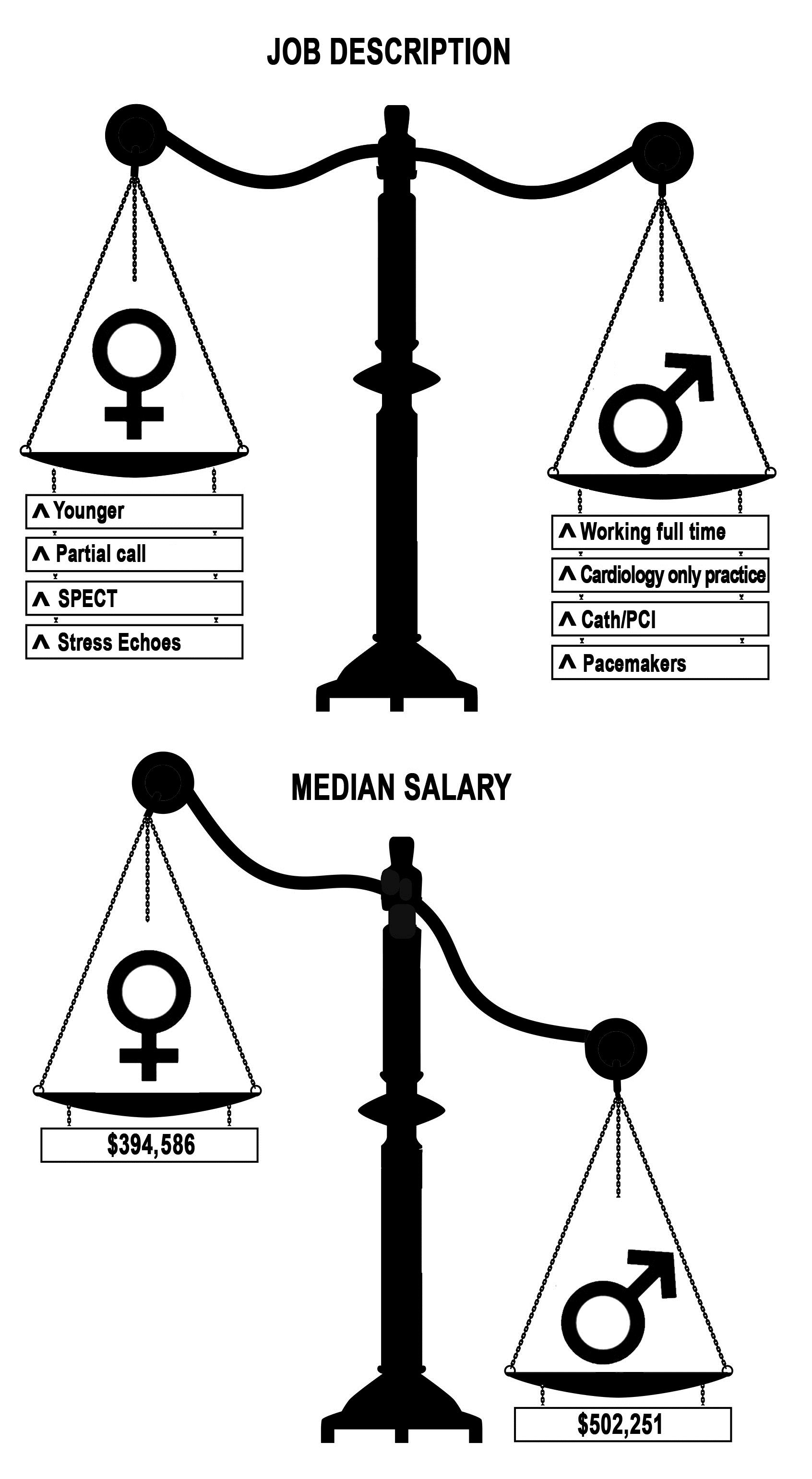
The researchers found that the ranks of women cardiologists remain disproportionally small compared to those in medicine overall; women who choose the field are much less likely to specialize in higher-paying interventional procedures; and women earn less, even when adjusting for the different types of work they do.
'These results recapitulate the salary differences that have been found among male and female physicians, lawyers, business executives, and others,” said Pamela Douglas, M.D., Geller Professor of Research in Cardiovascular Diseases at the Duke Clinical Research Institute. Douglas is senior author of the research, which is also being published in the Journal of the American College of Cardiology.
“Cardiology needs to be welcoming to women,” Douglas said. ”One way to do this is to acknowledge these differences and work toward correcting them.”
Douglas and colleagues analyzed data from 161 cardiology practices in U.S. communities surveyed in a 2013 report from MedAxiom, a firm that gathers and distributes data and business information specifically for cardiologists. The survey is considered a non-biased look at business practices, including hours worked, types of work performed, and pay rates.
The researchers found that:
· Women constitute about 12 percent of cardiology ranks, which is disproportionately low, given that half of medical school graduates are female.
· Women are more likely to specialize in general/non-invasive cardiology, with 53 percent pursuing this sub-specialty compared to 28 percent of men.
· Almost 91 percent of male cardiologists stated they work full time, while about 80 percent of women said they work full time.
· Men dominate in interventional subspecialties that perform higher-paying catheter-based procedures. More than 39 percent of male cardiologists reported an interventional subspecialty, compared to 11 percent of women.
· Men earn more money, even after accounting for all measured differences in job description, practice setting and productivity. Inherent in the measure of productivity are the known biases in the billing system known as the relative value unit (RVU), in which procedures are reimbursed by the federal Center for Medicare & Medicaid Services based on a score that accounts for the complexity, time and value of a service. Interventional procedures generally have higher RVU scores than cognitive services. As a result, men cardiologists generated a median 9,301 RVUs, while women generated 7,430.
· The different procedures, working hours and billing rates translate into higher earnings for men – a median of about $100,000 a year more for men than for women.
· Even adjusting for differences in the amount and type of work performed, women in cardiology make about $32,000 less per year than their male counterparts. Over a lifetime of work, this totals more than $1 million.
“This is the first study to show that although men and women cardiologists share the same specialty, they have markedly different job descriptions,” Douglas said. “Thirty-nine percent of men are interventionalists vs. 11 percent of women, and this sets the stage for higher compensation.”
“The differences in sub-specialization and practice were striking and merit note,” said Reshma Jagsi, M.D., associate professor at the University of Michigan and the study’s first author. “But it’s also important to note that the difference in compensation between men and women couldn’t fully be explained by differences in subspecialty, procedures, or the many other personal, job, and practice characteristics that we evaluated.”
Douglas said the study did not address the reasons why women steered to general cardiology rather than the interventional subspecialty, nor did it explain the differences in the workload. But the study authors suggest that the differences could stem from enduring gender inequities professionally and differences in choices in work/life balance.
“It’s important to be looking at this, because we as a profession are not having full access to our ‘talent pool’ of qualified internal medicine residents,” Douglas said. “That becomes a business and health care issue, as we increasingly recognize the importance of diversity among providers to optimizing patient care.”
In addition to Douglas and Jagsi, study authors include: Cathie Biga; Athena Poppas; George P. Rodgers; Mary N. Walsh; Patrick J. White; Colleen McKendry; Joseph Sasson; and Phillip J. Schulte.
IMAGE: Credit Mark Dubowski for Duke Medicine
- Fuente: endovascular.es
@2011 endovascular. Última actualización: 31-03-2014
